Healthcare Economist |
| Should hospitals pay for housing for ED frequent flyers? Posted: 22 Jun 2021 06:16 PM PDT That is one approach being explored in Philadelphia according to an article in Kaiser Health News. Using funding from Temple University, two Pennsylvania Medicaid health plans, and some grant funding, the Template University Health System:
The program is not cheap, however. It cost $28,000 per person. Nevertheless, according to a Kaiser Family Foundation study last fall, over half of states are implementing or expanding Medicaid programs that address social determinants of health. Not all interventions addressing social determinents of health have the anticipated impact. Consider the free rideshare program from another Philadelphia university and my alma mater, the University of Pennsylvania:
In short, addressing social determinants of health is a laudable goal. Finding the most cost-effective ways to achieve these goals, however, can be challenging in practice. |
| GAO report on prescription drug advertising Posted: 21 Jun 2021 05:13 PM PDT Medicare beneficiaries are largely elderly individuals, many of whom suffer from a variety of health conditions. Pharmaceutical manufacturers want these patients and their physicians to be aware of new medical treatments that become available (i.e., new approvals) as well as new uses for existing drugs (i.e., new FDA indications). Direct-to-consumer advertising (DTCA) is one way that pharmaceutical firms make consumers aware of these new treatments. Drug company spending on DTCA increased significantly in recent years, from $1 billion in 1997 to $6 billion in 2016. The Government Accountability Office (GAO) provides some details on drug advertising in their 2021 report Medicare Spending on Drugs with Direct-to-Consumer Advertising. The report answers 3 questions:
Data on DTCA spending came from Nielsen Media and information on each drug (e.g., approval year, indication, brand vs. generic, biologic vs. small molecule) came from FDA approvals. DTCA spending between 2016 and 2018 was highest for Humira, at $1.4 billion. Spending for neuropathic pain drug Lyrica was $913 million and spending for type 2 diabetes biologic Trulicity was $655 million. The report also finds that Medicare and its beneficiaries spent $324 billion on prescription drugs that were advertised (58% of Medicare drug spending) compared to $236 billion (42%) on drugs that did not have any DTCA expenditures. Unsurprisingly, DTCA advertising rose when a drug received a new indication and fell when generic competitors entered the market. In fact the GAO reports:
A key question is, did increased advertising lead to increased use of these medications? The answer is almost certainly yes (why would drug companies advertise if they didn’t work?), but it isn’t the only or likely even the primary factor.
Additionally, there is some reverse causality to consider as well. DTCA spending is likely not allocated randomly across drugs. Blockbuster breakthroughs like Humira (for immunologic conditions) and Keytruda (to treat a variety of cancers) are much more likely to have high DTCA spending in large part because they represented a large clinical improvements over the previous standard of care. Drugs that offer only marginal clinical benefits are likely to have much lower DTCA. Below are the top drugs in terms of Part B, Part D and DTCA spending. 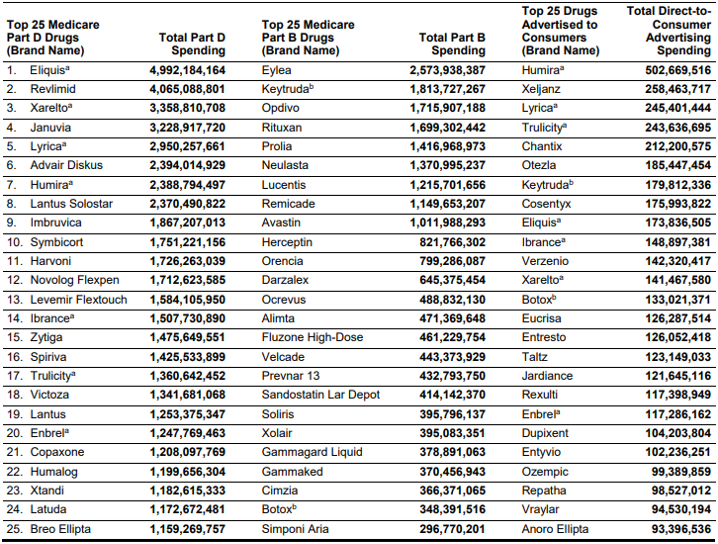 |
| You are subscribed to email updates from Healthcare Economist. To stop receiving these emails, you may unsubscribe now. | Email delivery powered by Google |
| Google, 1600 Amphitheatre Parkway, Mountain View, CA 94043, United States | |



No comments:
Post a Comment