The Magic used the top pick on Paolo Banchero, who became the fourth player from Duke to go No. 1 overall. Gonzaga's Chet Holmgren and Auburn's Jabari Smith Jr. then went to the Thunder and the Rockets, respectively.
This posting includes an audio/video/photo media file: Download Now
Kyrie Irving has a list of teams -- including the Lakers, Clippers, Knicks, Heat, Mavericks and 76ers -- that he'd like the Nets to work with on a sign-and-trade if he can't reach a new deal with Brooklyn.
This posting includes an audio/video/photo media file: Download Now
The G League Ignite has landed a commitment from forward Matas Buzelis, sources told ESPN's Adrian Wojnarowski. Buzelis,a 6-foot-10 forward, is the No. 11 player in the ESPN 100 for the Class of 2023.
This posting includes an audio/video/photo media file: Download Now
The Sixers are trading the No. 23 pick from Thursday night's NBA draft -- David Roddy -- as well as Danny Green to the Griz for De'Anthony Melton, sources said.
This posting includes an audio/video/photo media file: Download Now
Charlotte Hornets general manager Mitch Kupchak said he was glad to find out now rather than later that Kenny Atkinson felt uncomfortable being the team's head coach.
This posting includes an audio/video/photo media file: Download Now
The FDA is using its power to regulate tobacco products — ordering the vaping device Juul off the market and announcing its intention to lower the amount of nicotine in cigarettes and other products. Meanwhile, the Supreme Court rules on Medicare and kidney dialysis, and Congress makes progress on legislation surrounding guns and mental health. Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico, and Rachel Cohrs of Stat join KHN's Julie Rovner to discuss these issues and more. Also this week, Rovner interviews KHN's Noam N. Levey about the new KHN-NPR project on the growing impact of medical debt.
Plus, for extra credit, the panelists recommend their favorite health policy stories of the week they think you should read, too:
Cannabis News World posted: "What's new in weed: products and news from Wyld, Select, and more Marijuana.com With so many great cannabis brands releasing exciting new products in new markets, it can be hard to keep track of every release or event. So we're rounding up a few " Cannabis News World
What's new in weed: products and news from Wyld, Select, and more Marijuana.com With so many great cannabis brands releasing exciting new products in new markets, it can be hard to keep track of every release or event. So we're rounding up a few significant happenings in the industry. This week, we look at releases by Zig-Zag and more. Zig-Zag: new rose petal cones and wraps Cones shaped from rose petals? Look no further. Joint papers brand Zig-Zag just launched rose wraps and cones this month. Find the cones in packs of three and the wraps in packs of two. Available: Nationwide Cann: limited BOGO deal From May 1 - 31, Cann is offering a buy one get one free promotion on its core beverage products. Right now, you can buy one Hi Boy 4-pack of any core flavor, and get one Hi Boy 4-pack of any core flavor or buy one Cann 6-pack of any core flavor, and get one Cann 6-pack of any core flavor. Available: California, Illinois, Massachusetts, Nevada Find Cann Blazy Susan: new CBD line Smoking accessories brand Blazy Susan has released its new line of full-spectrum CBD products. Colorado-made and dubbed Susan's Own, you can find tinctures, bath bombs, muscle rubs, and gummies in varying CBD doses. Available: Nationwide Select: CBD Bites Select's CBD Bites line includes Snooze (blackberry flavor — 1:1 CBD:CBN), Chill (mango flavor — CBD), and Recover (watermelon flavor — 1:1 CBD:CBG). Buy them in-store or online. Available: Nationwide Find Select Seed & Smith: new infused pre-rolls Available in Colorado and packed in Zig-Zag papers, Seed & Smith has released its live-resin-infused pre-rolls in Lemon Cake, Midnite, Garlic Road, Super Sour Lemon, Purple Punch, and Chem De La Chem strains. Available: Colorado Seed & Smith Denver Seed & Smith Louisville Wyld: new sour gummy flavors Fans of gummy edibles can now find Wyld's sour…
uaenews4u posted: " Dhs500m investments "Binghatti Canal" the latest Banighatti Developers' project in Dubai's Business Bay *"Binghatti Canal" consists of 300 units and hand over starts in June 2023 Muhammad binghatti: - "Binghatti Canal" is our fiftie" Uae news 4u
"Binghatti Canal" the latest Banighatti Developers' project in Dubai's Business Bay
*"Binghatti Canal" consists of 300 units and hand over starts in June 2023
Muhammad binghatti:
- "Binghatti Canal" is our fiftieth project in Dubai and it will be a new shift in the company's portfolio
-We purse a local real estate brand that promotes our transition to globalization
-The new project reflects the inauguration of the smart real estate of the next generation
-Flexible payment systems suitable for all customers... and a discount of Dhs 300,000 on any unit in a one-day offer
-The real estate sector in Dubai attracts local and global investors with the improvement of market factors
Dubai - United Arab Emirates
June 24th , 2022
Binghatti Developers, the leading developer of affordable housing projects , and one of the most vibrant and popular UAE real estate developers, announced the launch of the "Binghatti Canal" in the Business Bay area, Dubai. An investments of DHs500m, the project will be completed in June 2023.
The announcement came during the great celebration held at the Grand Hyatt Hotel in Dubai on Wednesday, June 22nd , 2022, in the presence of a large number of their management team, main partners, investors and customers looking for buying housing units in the company's latest real estate projects.
The residential project, "Binghatti Canal", consists of 300 units, including 124 one- bedroom, 85 two-bedroom apartments, in addition to 84 studios, all are overlooking the most luxurious waterfront destinations in the Business Bay area with direct views of the center of the city of Dubai.
"We are pleased to add our 50th project in the company's portfolio in the United Arab Emirates, which will be a new shift in our real estate journey," said Muhammad Bighatti, CEO. "This innovative project, which will be constructed in one of the most prosperous areas of Dubai, is one of our many achievements for this year," he added.
"The project will be unique in terms of creativity and luxury, as it contains elegant and practical apartments designed in an exclusive contemporary style in classic designs with wonderful views of the Dubai Water Canal. The high standards of privacy and security add to its excellence," he said.
"Our architectural philosophy focus on the new generation of streamlined designs that extend from the stereotype to the dream house, while providing exceptional and unique facilities, especially the architecture of the facade , the distinctive classic colors and unique interior designs that make it distinct from others. The strategic location in Business Bay makes walking and commuting to all parts of Dubai an easy experience for residents," he added.
"Our smart homes provide comfort and the highest standards of security in a modern and luxurious lifestyle with high- tech solutions that facilitate the customers' lifestyle, especially with the integration of the virtual assistant system (Alexa) to facilitate daily household tasks," he said.
The apartments in the Binghatti Canal project with their comfort and luxury, the interior design of the spaces that offers a perfect balance between practical design and high technology, make it the ideal destination.
The CEO indicated that the company offers the new generation of real estate that includes smart systems in its projects without any additional cost. They succeeded in launching a local real estate brand famous for visual identity and has delivered about 25 towers in Dubai Silicon Oasis, 3 towers in Dubailand, 3 towers in the Al Jaddaf area, and two towers in the Business Bay area.
He noted that Binghatti Developer's plans focus on becoming global, while maintaining its competitiveness among the leading real estate developers in the Dubai market, which is full of attractive opportunities.
He revealed that the real estate market is on the trajectory of strong prosperity amid the recovery of the local economy, expecting this recovery to continue thanks to the UAE rational leadership and the new residency and citizenship regulations.
Binghatti confirmed that the company is the fastest real estate developer in Dubai in terms of handing over, as projects are delivered ahead of schedule. He praised the Dubai positive economic climate and the huge opportunities it provides to national and foreign investors.
The CEO stated that the company offered a discount of Dhs300,000 on any unit in "Binghatti Canal" in a one-day only offer, which is the same day of launching the project, while the providing flexible and attractive payment plans, which make the project an ideal option for investment.
The project includes units of different areas, as the unit spaces start from 93.09 square feet to 448.66 square feet, in addition to areas of 769.79 square feet, 778.66 square feet, and other units ranging from 234.19 square feet to 1377, 57 square feet.
The individual balconies intertwine with each other to form a unified view that distinguishes the "Binghatti Canal" mark from others.
The interior spaces were also carefully designed to the smallest details to ensure quality and design of the highest standards of function. The project includes private swimming pools for some private units, with the use of the best materials used in the finishes, such as Italian marble, in addition to high-end wood and gilded metals.
The "Binghatti Canal" is located in Business Bay, one of the most famous developed areas in Dubai. It is an integrated city within a city, which contains residential, recreational and commercial spaces, as it helps residents to easily move around and reach Dubai's tourist attractions and major famous destinations in a few minutes. It is close to central Dubai, the Meydan area and Jumeirah, and 5 minutes from Downtown, and 13 minutes from Dubai International Airport.
The project is also close to Dubai's tourist destinations, including City Walk, Yacht Club, Al Safa and La Mer Park, Kite Beach and Zabeel Palace. This all is added to its proximity to vital business areas in the emirate.
Business Bay is the core of Dubai's dynamic growth and success as a world-class city. The progressive vision of Business Bay is to create "Manhattan of Dubai" as it is the heart of the emirate, with its impressive mix of residential and commercial towers and modern entertainment venues.
=End=
About Binghatti Developers
Binghatti Developers is an award winning real estate developer in Dubai, headed by CEO and Chief Architect, Muhammad Binghatti. The dynamic company offers distinctive properties with refined architectural designs, world-class materials, and unparalleled lifestyle amenities. Empowered by commercial expertise since 1875, the brand strives to redefine the industry standards by delivering quality projects at affordable prices in a timely manner.
Binghatti's approach to development has allowed for the successful handing over of projects telate to some of the world's largest banks, hotel groups, and real estate funds, while also providing comprehensive solutions to end users. Within a short time frame, the company has proven itself as a viable alternative to some of the biggest reputable companies operating in in Dubai with an extensive portfolio of completed projects.
Binghatti Developers nowadays is working in several areas across Dubai including Business Bay, Dubai Silicon Oasis, Al Jaddaf, Dubai Marina, Jumeirah Village Circle, Liwan, and Dubai Land Residence Complex, in addition to a huge commercial project in Dubai covering an area of one million square feet. The company has bold plans to expand in the near future, with a particular focus on the growth of its real estate portfolio in Dubai.
I hope you've been well and are enjoying the beautiful summer we're having! While I'm sipping on some morning coffee and before I head out for the day, I wanted to share a few sales going on for some of my favorite products.
Simply Organic Bamboo 🐼🛏️
I recently updated the bedding in my bedroom (more to come on that!) and I chose a duvet cover that's made from 100% organically grown bamboo. It's softer than my previous one and is breathable for these warm summer nights. There are so many things that I like about this brand. They use eco-friendly and renewable bamboo, as well as eco-friendly shipping and packaging. I also love that they're OEKO-TEX certified, which means they're independently tested and shown to not have harmful levels of toxins.
Since we spend about a third of our day in bed (less if you're a mom with an infant!), I want to make sure it's healthy bedding.
This is the baby food that I wish I'd had when my kids were starting to eat solids! Their recipes mimic the macronutrients of breastmilk, offering the right balance of fat, protein, and carbs for babies over 6 months old. They only use grass-fed and pasture-raised meats from small American family farms that never use antibiotics, hormones, or GMO feed.
Their food pouches and puffs are perfect for on-the-go trips during the summer. I love that the pouches are lightweight for travel and they're more eco-friendly than bulky glass or plastic jars. And as always, the ingredients are high in healthy fats and low in sugar. If your little one still isn't big on solids yet, they also have a toddler formula made with grass-fed A2 milk that's packed with probiotics and other nutrients.
Do you have friends who'd love the Wellness Mama newsletter too? Share your unique referral link (below) and get the chance to win some of my favorite Wellnesse personal care products!
Bruce Drum posted: " In May, Norwegian and Boeing announced an agreement in principle for the purchase of 50 Boeing 737 MAX 8 aircraft with options for another 30 aircraft. Norwegian announced that the various closing conditions related to agreement have been met. F" World Airline News
In May, Norwegian and Boeing announced an agreement in principle for the purchase of 50 Boeing 737 MAX 8 aircraft with options for another 30 aircraft.
Norwegian announced that the various closing conditions related to agreement have been met.
Following this, Norwegian estimates that it will record a net gain of approximately NOK 2 billion in the second quarter of 2022.
Additionally, Boeing and Norwegian have filed to settle all outstanding legal disputes.
Cannabis News World posted: "Cannabis can help reduce fatigue, findings from a three-year-long study suggest Growth op More than 90 per cent of participants reported reduced fatigue following self-administered weed sessions. Excerpt only ... READ MORE BELOW Source : Cannabi" Cannabis News World
Cannabis can help reduce fatigue, findings from a three-year-long study suggest Growth op More than 90 per cent of participants reported reduced fatigue following self-administered weed sessions.
Curt Mekemson posted: " Peggy and I found this interesting rock formation looming above the petroglyphs that we located in the eastern section of Zion National Park. It was only the beginning of unusual rock structures that defined the area. I quickly learned when I was" Wandering through Time and Place
Peggy and I found this interesting rock formation looming above the petroglyphs that we located in the eastern section of Zion National Park. It was only the beginning of unusual rock structures that defined the area.
I quickly learned when I was a Peace Corps Volunteer in West Africa that my reality was substantially different from that of the tribal students I was teaching. It was a lesson that has served me all of my life. The human mind is incredibly flexible and our reality, to a large extent, depends upon what we are taught. Given my 1965-67 experience in Liberia, I can't even start to imagine what people believed 7,000 years ago.
That's when humans first started wandering the area now known as Zion National Park. They started with Archaic peoples, moved on to the Anasazi and Fremont cultural groups, and, in turn, were followed by the ancestors of modern day Native American Paiutes. Any or all of these groups may have left petroglyphs in the slot canyon Peggy and I explored in the eastern section of the Park. And all of them reflect thinking that we can only guess at.
Peggy and I are fascinated by petroglyphs, both from the connection it gives us to people from hundreds or even thousands of years ago, and from the unique look of rock art. We have visited sites throughout the Southwest. There is a certain commonality to the rock art depending on the culture represented. We have also found a similarity to sites selected by the ancients to leave their messages. Not surprisingly, they tend to be near water, which is where the people lived. But there was also an inclination to select locations that stood out from the surroundings. Possibly it gave a sense of sacredness to the area.
The site we visited was an excellent example of this, as our photos show. The strangeness, however, started with the directions to find the site. As I remember them: "Go down into the canyon and find a sand wash. Follow the wash up the canyon until it comes to the tunnel under the road. Go through the tunnel and follow the wash until you come to a trail to your left." There was as much room for interpretation in following the directions as there was for interpreting what the petroglyphs meant!
Our photos start with the tunnel.
It was appropriately hidden by trees and bushes.The sandy wash led right to it, however. The light we could see on the right suggested that the tunnel was a few feet long. (Photo by Peggy Mekemson.)Reality was different. It was much longer than it appeared to be. Fortunately, there was a light at the end of the tunnel.Peggy walked toward the light and disappeared. She boldly went forth where numerous others had obviously travelled, judging from the foot prints in the sand. But did they ever return? Maybe a little Sci-Fi/Horror movie music is called for here.She was waiting for me in the sandy wash that led onward, supposedly toward a trail that would lead off to the left and petroglyphs. We quickly learned that there were several trails leading off to the left where people had gone in futile searches! Fortunately, Peggy and I had an advantage...We were looking for an area that suggested the presence of petroglyphs. This rock structure seemed a likely candidate. We started looking for a trail to the left, and found even more interesting rocks.Peggy caught this photo and the following one.Photo by Peggy Mekemson.How's this for unusual? If I were a shaman, I'd think this would be a great location for petroglyphs.This fellow was not a petroglyph but part of the rock face, so to speak. I've learned a new word, BTW: pareidolia, the tendency to read into patterns and interpret visual stimuli, even when there is no intentional meaning present. A lot of that happens in my blogs. (Photo by Peggy Mekemson.)There was something surreal about the beauty of the area. (Photo by Peggy Mekemson.)I looked up and caught this colorful view.And then we reached the site. It was just beyond the green shrubs if my memory serves me correctly. It's hard to imagine a more stunning location. We were prepared to enter the alternate reality suggested by petroglyphs.The petroglyphs were waiting. This is obviously a human like figure, probably a woman, but what's with the strange diagram underneath? Does it represent power lines reaching out to the universe from the individual. I stared at it for a while and wondered if it didn't represent a reflection in water. Or a moon shadow. Remember the song by Cat Stevens? (Photo by Peggy Mekemson.)Another reflection shot? A selfie? Or possibly a mating couple. Such images are not uncommon in petroglyphs.This is frequently thought of as being an origin petroglyph, representing the entry into this world from another world. This panel clearly represents petroglyphs created in different times with the figures in the upper right being of more recent origin. Are they hiking with packs? Or are they paddling a boat? The wavy line may represent a lake and a stream. Or a snake? The lower guy on the right seems to be asking the question while the guy on the left seems to be running like crazy to escape. (Photo by Peggy Mekemson.)I labeled this guy as a moose. Why not— even though there is no record of moose in the Park area except in 2013 when one showed up. Tourists were told to keep their distance. We've found women portrayed like this throughout the Southwest. The circular figure may be the sun. I wondered if the wiggly lines represented counting, or a snake, or a river. Or...My imagination placed this woman on the warpath! (Photo by Peggy Mekemson.)
There were many other petroglyphs. At the end of the panels, Peggy and I found steps carved into the canyon wall leading up to a ledge.
I thought it might be interesting to climb up them and explore the ledge. Peggy felt it best that her 79 year old husband be grounded. Grin.
Wandering up the trail in search of more petroglyphs, we found a dead big horn sheep that may have slipped while climbing the walls. Or been taken out by a cougar.
It did not look very happy. Peggy wondered why I wanted to photograph it and decided it was a sign that we should turn around. Admittedly, it did look a bit Satanic...
Shortly afterward we came to what was obviously the end of the trail unless we wanted to scramble over rocks. We turned around leaving the sheep, the petroglyphs, the beautiful canyon and the tunnel behind. It had been quite an adventure. In my next post we will explore more of the unique beauty of East Zion National Park.
Passion for food & Travel! posted: " A rich savory chicken dish perfect served on a bed of past or on the side of a beautiful refresh salad! Prep Time: 15 min Cook Time: 25 min Serves: 4 Ingredients 2 tablespoons extra-virgin olive oil 4 medium chicken breasts, bon" Food Is What We Do!
Yes, Juul e-cigarettes have been banned in the US, but we talked about that yesterday. But what's like vapes? Replicants and '80s sci-fi? Maybe not, but anyway, Nightdive Studios has finally released Blade Runner: Enhanced Edition for Windows PCs (via Steam), PlayStation, Switch and Xbox consoles. The modernized version runs at 60 frames per second instead of the original's 15 fps, complete with updated animations and models.
At the time, Westwood's 1997 game pushed the boundaries of both graphics and gameplay. Instead of the usually fixed plot, Blade Runner changed the replicants and humans around with each playthrough while also offering branching storylines.
Rather than relying on either 2D art or crude 3D, the title used voxels (pixels with 3D attributes), giving far more visual detail for the era, including volumetric lighting. Think of it as the ray-tracing of '90's gaming. This choice in graphics technology made for a challenging remaster, however, as it didn't play well with graphics cards, and then the source code was lost in an office move. For those that played the unlicensed version, it might not look quite as good, but hey, at least it runs on your Switch.
As teased yesterday, the FDA has banned e-cigarette maker Juul from selling and distributing its products in the US. It ordered the company to remove its wares from the market or face enforcement actions. Juul told Engadget it intends to seek a stay on the decision. It's exploring all other options, including an appeal.
Slimmer, high-resolution phone cameras are incoming.
Despite featuring some of the smallest pixels yet, Samsung's new 200-megapixel camera sensor has autofocus capability in every pixel, binning for better low-light capability and multi-gain ISO for maximum dynamic range.
Each pixel has autofocus detection capability, and the Super QPD tech uses a single lens over four pixels for quicker and more accurate autofocus. It can also bin four 0.56 micron pixels into a larger 1.12 micron 50-megapixel sensor for better low-light capability, or even combine 16 pixels into one 2.24 microns in size.
A prototype of the EV showcases at the Goodwood Festival of Speed.
Polestar
The Polestar 5 is making its first public appearance at the 2022 Goodwood Festival of Speed in West Sussex, England. As part of the First Glance vehicles event, a prototype of the upcoming four-door electric GT sports car will drive up the Goodwood hill twice each day. The Polestar 5 is the production version of a concept EV called Precept, introduced back in 2020. When the company announced it was going to turn the concept into a real vehicle, it said it would manufacture the EV at a new carbon-neutral facility in China.
The company previously cut 150 jobs in May amid business woes.
Netflix has laid off around 300 people in its latest round of job cuts. Most of the layoffs were in the US, according to Variety, and affected a number of departments. This is Netflix's second round of layoffs due to slowing revenue growth. It laid off 150 employees, along with many part-time workers and contractors, back in May. The company has around 11,000 employees globally. Netflix is still hiring on other fronts and has already earmarked around $17 billion to invest in content this year alone.
This comes after the website launched its own NFT collection in May.
eBay has truly (unfortunately?) fully embraced non-fungible tokens: The e-commerce company has acquired KnownOrigin, an established marketplace for digital art NFTs. KnownOrigin has been around since 2018 and gives artists a platform to create and sell their art as NFTs in exchange for cryptocurrency payments.
theorkneynews posted: " The UK's Office of National Statistics reports that (25.06.2022): The percentage of people testing positive for coronavirus (COVID-19) increased in all UK countries in the week ending 18 June 2022 (17 June for Scotland). The increase was likely cau" The Orkney News
Guest Blogger posted: " Image by White77 from Pixabay By Anita Ginsburg While your children are probably greatly enjoying their summer vacation, it's never too early to start planning for the school year. While we tend to think of planning for the school year in terms of" Michigan Mama News
While your children are probably greatly enjoying their summer vacation, it's never too early to start planning for the school year. While we tend to think of planning for the school year in terms of buying school supplies and new clothes, there are also other very important things you must get done as well. Below are some of the different kinds of appointments you should make for your children before they go back to school.
Dietitian Visit
This might seem kind of different, and it is. That is exactly the point, actually. Visiting a dietitian can help your child understand what foods are healthy and what ones are not. In today's world, our food is extremely low in quality, so teaching your kids how to eat healthy has never been more important. The dietitian will be able to give you ideas on how to stay healthy by eating better.
Dentist Appointments
Your children's dental health is also very important. Damage done to your teeth can have serious repercussions even during youth. Children and teens may also experience certain dental issues that should be addressed early to help preserve their teeth for adulthood. Make sure to make dental appointments for all your children before school starts. This will allow you to get them out of the way while you still have open schedules during the summer. It will also help protect your children's teeth. Especially since they will not typically be able to brush, rinse, or floss while at school.
Doctor Check-Ups
You should also schedule check-ups for your children before school starts as well. In all likelihood, your children will be given the thumb's up in regards to their health. Still, there is a chance that health issues you have not noticed before will be detected during the check-up. This can allow you to address such health problems well before school starts again. That way, your children will be able to focus more squarely on learning.
Vision Check-Ups
Similarly, you should take your children to an optometrist before school begins. You should know exactly how good your children's eyesight is before school. Good eye sight of course is needed to excel in school due to all the reading and writing required. Make sure your children get glasses if they need them.
Make sure your children attend these and other important appointments. Doing so can help protect your children's health. That way, you'll have less to worry about as a parent, and your children can focus on learning instead of health-related issues.
About the Author
Bio: Anita is a freelance writer from Denver, CO. She studied at Colorado State University, and now writes articles about health, business, family and finance. A mother of two, she enjoys traveling with her family whenever she isn't writing. You can follow her on Twitter @anitaginsburg.
Cannabis News World posted: "New Mexico Cannabis Control Division Lifts Cease and Desist Order from Producer Involved in Medical Cannabis Recall Cannabtimes <![CDATA[The New Mexico Cannabis Control Division (CDC) has lifted a cease and desist order from a producer that was inv" Cannabis News World
New Mexico Cannabis Control Division Lifts Cease and Desist Order from Producer Involved in Medical Cannabis Recall Cannabtimes <![CDATA[The New Mexico Cannabis Control Division (CDC) has lifted a cease and desist order from a producer that was involved in a medical cannabis recall last month.Regulators allowed Santa Fe-based Sacred Garden to resume operations April 27, after the operator remedied or initiated plans to remedy violations previously cited by the CDC, according to NM Political Report.The CDC issued the cease and desist order and a product recall March 24, after investigating patient complaints about mold found on Sacred Garden's products.RELATED: New Mexico Issues Recall of Medical Cannabis Products from Sacred GardenThe investigation uncovered conditions at Sacred Garden's that regulators said would pose a risk to the public, according to NM Political Report.Sacred Garden filed a request for an injunction days after the CDC issued the cease and desist order to block it, the news outlet reported. A state district judge initially ordered regulators to allow Sacred Garden to sell manufactured products, such as edibles, until its facility was deemed safe to fully reopen, and criticized the CDC in a subsequent hearing for not outlining clear steps for the company to remedy its violations.Ultimately, the judge gave the CDC roughly a week to establish and complete a testing regime, and six of the 13 samples from Sacred Garden that were tested showed high levels of yeast and mold, according to NM Political Report.The lab results revealed that some of Sacred Garden's cultivars had tens of thousands of colony forming units of yeast and mold per gram, according to the news outlet, while others showed levels as low as 45 colony forming units of yeast and mold per gram.The cannabis testing standards approved and adopted by the CDC mandate that all cannabis flower is tested for aspergillus, a type of fungus that can produce mycotoxins, but there are no testing regulations…
Pit posted: " Reh-Fütterung im Garten hinter unserem Haus: 360-Grad 3D Video In the meantime, I have managed to upload the video shot with my new INSTA360 ONE RS to YouTube in such a way that it can actually be played as a 3D video. However, the image quality is no" Pit's Fritztown News
Reh-Fütterung im Garten hinter unserem Haus: 360-Grad 3D Video In the meantime, I have managed to upload the video shot with my new INSTA360 ONE RS to YouTube in such a way that it can actually be played as a 3D video. However, the image quality is not as good as in my first video […]
Sickr posted: " The latest physical Japanese video game software and hardware charts are in via Japanese sales tracker, Famitsu. There's a new No.1 video game this week which has dethroned the unstoppable Nintendo Switch Sports in the land of the rising sun and it is De" My Nintendo News
The latest physical Japanese video game software and hardware charts are in via Japanese sales tracker, Famitsu. There's a new No.1 video game this week which has dethroned the unstoppable Nintendo Switch Sports in the land of the rising sun and it is Demon Slayer: Kimetsu no Yabia - The Hinokami Chronicles which shifted 20,964 […]
So, you're American, you have a lousy health insurance plan, you get cancer. You survive cancer. But can you survive your massive medical $$$ debt?https://t.co/e6Jzw9W4SR
I read your investigation about health care and debt on NPR’s site (“Diagnosis: Debt: 100 Million People in America Are Saddled With Health Care Debt,” June 16). However, it seems the story’s focus is wrong. It shouldn’t be about how we pay for these astronomical medical bills but why are they so high to begin with? How do hospitals get away with their fees? For example, my daughter, who is 7, has been to the hospital/emergency room five times in her life. Each bill has been completely different with no rhyme or reason. The latest one was $7,000 for about a three-hour ER visit and for two IVs! It’s the highest bill we have ever seen, and that includes a two-night stay at a hospital. In addition to this bill, collections called us — and it hadn’t even been 60 days since our visit and had been only a few weeks since the hospital visit. So now our credit score could be affected, and we haven’t even had a chance to review or figure out how to pay this bill. Would love all this explained.
— Ilyssa Block, Kansas City, Missouri
A Hard-Learned History Lesson
Although I liked the article by Noam N. Levey and Aneri Pattani on people burdened by medical debt (“Diagnosis: Debt: Upended: How Medical Debt Changed Their Lives,” June 16), it uses the term “grandfathered in.” This term was used as a rule to prevent Black people from voting after the Civil War. Please make an effort to refrain from using this offensive term.
Every month I see and hear these “Bill of the Month” stories on NPR’s webpage or broadcast on the NPR affiliate station in my area (“Her First Colonoscopy Cost Her $0. Her Second Cost $2,185. Why?” May 31). Every month I pat myself on the back for having decided that there is no way I am ever going to put myself through so-called screenings, which are just one more avenue for the U.S. health delivery system to screw people over as that health delivery system is well aware that there is no oversight for this type of predatory billing. I can tell you at my age and with only Social Security retirement as sole income, I couldn’t ever hope to hire legal help to dispute a bill like those featured in “Bill of the Month” — a bill like that would either cause me to have an immediate heart attack or file bankruptcy or both. Nope. No screenings. I actually have decided that, if I have any choice in the matter, I will simply forgo any so-called medical care. Obviously, if I keel over and pass out and someone hauls my sorry self into the emergency room, I won’t have the choice (except to walk out once “revived”). Given the state of health care and the predatory behaviors of the bottom-lining money-hungry hospitals, clinics, and even just doctors, my choice is simply to opt out. KHN needs to use its voice to tell the U.S. medical community that people are so tired of the garbage that they simply refuse care.
— Jan Baldwin, Coburg, Oregon
First colonoscopy: $0Second colonoscopy: $2kAnother example of how the fine print can put patients on the hook for bills that should be covered, especially in this case of a preventative screening. Patients deserve better.https://t.co/v55XVdGAeB
In Michelle Andrews’ story about unexpected costs after a polyp removal during a colonoscopy, she states the anesthesiologist “merely administers a sedative.” This is an understatement. Anesthesiologists perform a review of the patient’s chart, see the patient pre-procedure, monitor their vitals during the procedure, and assess them post-procedurally. Furthermore, anesthesiologists are prepared to manage unexpected emergencies, including unexpected aspiration, allergic reactions, cardiac arrest, etc. This is more than “merely administering a sedative.”
We keep folks from dying or having complications and train a long time to do so. The flippant manner in which our actions are framed in the article is unfortunate.
As president of the American Society for Gastrointestinal Endoscopy, I listened with interest to a recent segment on “All Things Considered” regarding patient cost sharing for a screening colonoscopy. The segment featured patient Elizabeth Melville, who received a bill for her screening colonoscopy that involved a removal of a polyp.
I was dismayed by the segment, which included several factually incorrect and misleading statements by Dr. Elisabeth Rosenthal, and which were incredibly damaging to efforts to eliminate impediments and misinformation about screening colonoscopy. ASGE has been at the forefront of policy efforts to eliminate patient out-of-pocket costs for screening colonoscopy, including those screenings that involve the removal of a polyp or other tissue. As the segment correctly noted, the Affordable Care Act provides for coverage without patient cost sharing of preventive services that have an “A” or “B” rating from the U.S. Preventive Services Task Force, which includes colorectal cancer screening. Recognizing that colonoscopy is the only cancer screening modality that also allows for actual removal of precancerous lesions in real time (and thus preventing the cancer), it is particularly important that patients and consumers understand the facts.
Following passage of the ACA, legislative and regulatory corrective actions have been necessary to ensure that patients who undergo a screening colonoscopy that includes a polyp removal are not stuck with a surprise bill. As noted, screening colonoscopy is a unique preventive service in that it not only detects cancer, but it can prevent it through removal of suspicious or potentially precancerous polyps or lesions. In 2020, Congress passed legislation that would phase out by 2030 cost sharing for Medicare beneficiaries when a screening colonoscopy turns diagnostic during the screening encounter. That means, if a Medicare beneficiary has a screening colonoscopy today and a polyp is removed, that patient is likely to have an out-of-pocket payment obligation.
The difference in cost-sharing rules for commercially insured patients and Medicare beneficiaries has created confusion for patients, and the changes in regulation have created complex billing scenarios. Dr. Rosenthal referred to billing for colonoscopy as a “gray area.” This is not a gray area to ASGE, as coding rules are clear. But there are scenarios that could impact whether a patient has an out-of-pocket obligation for a colonoscopy. For example, often insurers will not cover a screening colonoscopy without cost sharing if the screening occurs less than 10 years after the patient’s previous colonoscopy. These shorter screening intervals typically occur when a patient is considered high-risk, or if there was a finding during the previous colonoscopy, such as a polyp, as used in your illustration. Many insurers regard these colonoscopies as “surveillance” or “high-risk” colonoscopies and will not cover them as a preventive screening without cost sharing. This is not the decision of the physician or hospital; this is a decision made by the insurance company.
I was particularly struck by Dr. Rosenthal’s comment that “it is not OK to change the game in the middle of the test,” which leads to a patient getting a bill. I want to be very clear that when a patient is scheduled for a screening colonoscopy, the physician performing the colonoscopy has no idea whether a polyp or tissue will be found and will need to be removed. This is not a “gotcha” game that physicians are playing with patients, as insinuated by Dr. Rosenthal’s remarks; there are coding and billing rules that must be followed when facilities and physicians are submitting claims to insurance companies. ASGE continually works to ensure that we educate and promulgate coding rules and updated guidance for our 15,000 members worldwide.
The cost-sharing policy for colorectal cancer screening, and screening colonoscopy specifically, is complex and confusing. We are disappointed that NPR did not use the segment as an opportunity to work through the complexity to provide consumers with a better guide of questions to ask their insurance company before scheduling a colonoscopy, including whether a screening colonoscopy performed at an interval of less than 10 years will be covered under their health plan without cost sharing.
— Dr. Bret T. Petersen, ASGE president, Rochester, Minnesota
Great Bill of the Month reporting today by @mandrews110 for @KHNews. Nobody likes getting a colonoscopy. Patients shouldn't be penalized for doing the right thing and getting recommended cancer screenings: https://t.co/cNlEj85IZ4
I spoke with @hnorms from @KHNews about the state of the pandemic and health equity. There is still a lot to be done to movement smart policies that help high risk communities of color. https://t.co/LAf2WCIN0X
This article is grossly inaccurate and insulting (“The New MADD Movement: Parents Rise Up Against Drug Deaths,” May 23). Most fentanyl users are not all-star athletes or honor students. Their parents are not more educated than the parents of addicts. And the parents of addicts have been mobilized for years, with many feeling that the fentanyl movement has distracted attention away from needed health care. The article says that the drugs are being introduced by Mexican cartels that seek vengeance against low-level dealers, many of whom are just friends getting things for one another. The article distinguishes between drug users and fentanyl “victims,” creating and reinforcing the stigma these groups claim to be trying to eliminate. It does a great disservice to those of us who lost children to addiction and overdose, and is insulting to our children and to us as parents. Thank you.
— Susan Elamri, Detroit
Interesting read detailing the lack of accountability for drug dealers selling fentanyl laced counterfeit pills resulting in death/overdoses. Consequences and rehabilitation should not be mutually exclusive solutions, we can do both. https://t.co/KlvBH3O1kq
— Chief Paco Balderrama (@BalderramaPaco) May 23, 2022
— Paco Balderrama, chief of police, Fresno, California
Perhaps the answer is to change the scale of weight. Why do 25% of adults get to be called “normal” and 75% of adults are “overweight”? Let’s base the decision on reality-based observation!
— Leslie Rigg, Lake Worth Beach, Florida
1) Anti-fat bias is real and certainly an issue. For physicians and others who treat people with #obesity, the question becomes where to draw the line. 'Almost Like Malpractice': To Shed Bias, Doctors Get Schooled to Look Beyond Obesity https://t.co/ap127widIs via @khnews
“These children already face tremendous challenges, having been given up by their parents voluntarily or removed from their homes due to abuse, neglect, or abandonment.”
Sometimes, of course, that’s true. But no reporter would write that every person in jail is a criminal. Many are awaiting trial and can’t make bail. Similarly, children can be in foster care for weeks, even months before any court ever determines if they have been “abused” or “neglected.” Until then, they are in foster care because their parents have been *accused* of abuse or neglect.
(Also, by the way, neglect laws are so broad and vague that often what the parent really is guilty of is poverty — but that’s another issue.)
— Richard Wexler, executive director of the National Coalition for Child Protection Reform, Alexandria, Virginia
[Editor’s note: Thanks so much for your insight. The article has been updated to reflect that the parents are absent “due to accusations of abuse, neglect, or abandonment.”]
.@sclaudwhithead looks at "hoteling," Georgia's practice that makes high-need foster kids sometimes sleep in hotels or offices. The pandemic made the problem worse, but state lawmakers spent more to try to pay extra for foster parents to take kids. #gapolhttps://t.co/xRXbKCSVEM
Key to Harm Reduction: Buy-In From People With Addiction
With overdose deaths skyrocketing to never-before-seen levels, the United States needs harm reduction strategies to protect the health and wellness of Americans. In 2020, 41 million Americans needed substance use treatment within the previous year; however, of those who needed such treatment but did not receive it at a specialty facility, a staggering 97.5% did not feel they needed it. Although America has a troubling treatment gap exacerbated by systemic legal and regulatory barriers to evidence-based addiction care, most people who need substance use treatment don’t want this treatment as it is currently being offered.
To support our friends and family members living with addiction, our system must also embrace harm reduction approaches that engage people who use drugs (PWUD) before they are ready for abstinence-based treatment (“As Biden Fights Overdoses, Harm Reduction Groups Face Local Opposition,” June 14).
Harm reduction saves lives. Drug checking services and naloxone distribution prevent overdose deaths, while syringe and related service programs help stop the spread of infectious diseases such as HIV/AIDS and hepatitis. These are all worthy ends in themselves, but harm reduction has the further benefit of building a meaningful alliance between health care professionals and PWUD. With this therapeutic relationship, PWUD have facilitated access to high-quality, evidence-based treatment and services when they become ready for this help. It’s an obvious point, but too many people overlook the fact that a person can’t receive treatment or enter recovery if they’re dead.
As a physician, I swore an oath to do no harm — not to do nothing. Failing to embrace and expand harm reduction efforts, by definition, leaves too many of our friends, family members, and loved ones at an unacceptable risk of dying. The dichotomy between offering more addiction treatment and providing PWUD with the tools they need to live healthier lives is a false choice. The United States must simultaneously invest in treatment expansion and increase the availability of low-threshold harm reduction services; otherwise, I fear the country’s addiction and drug overdose crisis will continue to get worse.
— Dr. Brian Hurley, president-elect of the American Society of Addiction Medicine’s Board of Directors, Los Angeles
1. Distribute the drug solely by the government, ensuring its purity, proper dosage, and safe setting for the user, providing real-time overdose care and optional consulting for anyone who wants to quit, all for free.
2. Make some nonaddictive antidepressants (generally SSRIs, or selective serotonin reuptake inhibitors) less restrictive. You know, how health care in your country is expensive, visiting a psychiatrist or psychologist, refilling, blah-blah. I know, the nation who can’t agree on banning AR-15s from being sold to 18-year-olds won’t agree on this.
What if you let people have some SSRIs over the counter? These are not recreational, are generally safe (way safer than opioids), and do help with anxiety. Hey, what drives people to opioids? Aren’t anxiety levels at their highest all across the globe?
Also, the drugmaker mafia will support it.
Just as we have embraced over-the-counter drugs for widespread diseases like colds, we might adopt the same concept in mental health care as well. Anxiety is becoming more widespread compared with colds (my gut says).
Very few cities pass the World Health Organization’s unrealistic threshold of 5 micrograms per cubic meter, and why would you get a mechanical engineer to provide input on environmental issues? Why, because the real environmental specialist said this was not an issue? As for dust on a picnic table, that is a horrible example. We get dust on our picnic table anytime the wind blows, and we don’t live by a mine. Maybe WHO should recommend that the wind stop blowing because it causes dust.
From the WHO’s website: “In 2019, 99% of the world population was living in places where the WHO air quality guidelines levels were not met.” This is not a reasonable standard and was selected by bureaucrats that are out of touch with life and the real world. All of the real information and statistics say there is not a problem, but your article makes a problem where one does not exist and people who are not willing to fact-check you will think there is a problem. All these people with health issues are unfortunate and that’s very sad, but people everywhere have sad health issues. Stick to the scientific facts and real monitoring numbers, and don’t drag “The Sky Is Falling” people into news articles. Facts matter!
— John Utaz, Salt Lake City
Cultivating an interest in 'dusts’ at the moment and this article includes extractive industries/ mining. https://t.co/JsXCA7rxkD
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
The FDA this week launched a crackdown on smoking and vaping — ordering the vaping device Juul to be taken off the market and announcing its intention to require makers of cigarettes and other tobacco products to reduce the amount of nicotine in them.
Meanwhile, the Supreme Court did not announce a ruling in a high-stakes abortion case, but it said that private health insurers could limit the amount of kidney dialysis care they provide, thus forcing some patients onto Medicare.
This week’s panelists are Julie Rovner of KHN, Joanne Kenen of the Johns Hopkins Bloomberg School of Public Health and Politico, and Rachel Cohrs of Stat.
Among the takeaways from this week’s episode:
The FDA has ordered Juul to remove its e-cigarettes from the U.S. marketplace because the company’s application to the agency did not provide enough information for regulators to determine whether Juul presented a hazard to users. The FDA said there were concerns about the risk of some harmful chemicals leaching from the Juul pods. Juul is expected to appeal the FDA decision to the courts.
Juul helped ignite an explosion in e-cigarette use when it came on the market, and officials originally thought it would aid smokers seeking to kick the cigarette habit. But the industry’s use of flavored tobacco and aggressive marketing helped fuel a dramatic rise in use among teens and led to a regulatory crackdown.
The Supreme Court this week ruled that employers may opt to make all dialysis treatment out of network in their workers’ health plans, a decision that would likely drive many patients to seek Medicare coverage for their kidney problems. The decision was a disappointment for dialysis providers, who receive less in reimbursements from Medicare than they typically get from private insurance plans.
The decision leaves many details unresolved and further legal fights could be coming. Dialysis providers might also turn to Congress to establish laws that would prohibit employers from such moves.
The Senate is likely to consider a bill proposed by Sens. Susan Collins (R-Maine) and Jeanne Shaheen (D-N.H.) that seeks to lower the cost of insulin. The bill is considered more friendly to drugmakers than another measure that passed the House this year. The Senate bill seeks to get drugmakers to offer insulin at the price they received from Medicare in 2021 by allowing them to bypass rebates and other costly subsidies paid to pharmacy benefit managers and insurance plans. It would also limit out-of-pocket costs for insured consumers to $35.
As the Senate moves closer to a vote on gun safety legislation, other efforts are underway to find more funding for programs to help deal with mental health problems. Those efforts could help with campaigns to reduce suicides and domestic violence, which are also often tied to guns.
The House is launching efforts to pass appropriations bills, and the initial funding measure for the Department of Health and Human Services once again does not include the so-called Hyde Amendment, a long-standing policy named for the late Rep. Henry Hyde (R-Ill.) that bans federal funds from being used for most abortions. Earlier efforts by the House to jettison the Hyde Amendment did not clear the Senate.
President Joe Biden has nominated Arati Prabhakar, former head of the Defense Advanced Research Projects Agency (DARPA), to head the White House Office of Science and Technology Policy. She would replace Eric Lander, who was forced to resign after reports of staff harassment.
Prabhakar appears to be a noncontroversial choice and comes with a good deal of management experience. Her responsibilities will likely include overseeing pandemic planning, efforts to shape a new biomedical research agency called ARPA-H, and strategies to enhance cancer prevention.
Also this week, Rovner interviews KHN’s Noam N. Levey about the new KHN-NPR project on medical debt, called “Diagnosis: Debt.”
Plus, for extra credit, the panelists recommend their favorite health policy stories of the week they think you should read, too:
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Armando Peniche Rosales tiene un dedo del pie torcido, que durante años ha pronosticado el clima y se vuelve sensible cuando se avecina lluvia o frío.
“Nunca se curó bien”, dijo Peniche Rosales, quien se rompió el dedo medio del pie izquierdo hace años cuando era jugador de fútbol en una escuela secundaria de Denver, y regresó cojeando a su casa sin ver a un médico.
En ese momento, estaba viviendo en los Estados Unidos sin papeles. Desde los 9 años, cuando se mudó a Denver, hasta los 20, no tuvo seguro médico.
El dedo del pie es un pequeño recordatorio de los momentos en que su familia sintió que tenía que “elegir entre su salud o su futuro” en el país, dijo Peniche Rosales, que ahora tiene 35 años. Ambos padres enfrentaron esa decisión.
Su madre eligió su propia salud, regresando a México para recibir tratamiento por migrañas y una afección de la tiroides, aunque eso significara pasar una década separada de su familia. Su padre eligió su futuro, trabajando largas semanas con síntomas que las clínicas gratuitas le dijeron que eran hemorroides pero que en realidad era cáncer de colon.
El padre de Peniche Rosales ahora está enterrado en un cementerio de Denver con vista a las Montañas Rocallosas.
“Está descansando en su hogar, como él quería”, dijo Peniche Rosales. “Amaba las montañas”.
A nivel nacional y en Colorado, la proporción de personas sin seguro médico ha sido durante mucho tiempo significativamente más alta entre los hispanos que entre los residentes blancos, negros o asiáticos no hispanos. Los inmigrantes que no tienen estatus legal, y aquéllos que tienen residencia legal pero cuyas familias tienen un estatus migratorio mixto, constituyen una gran parte de ese grupo.
Colorado recientemente hizo que algunos de ellos fueran elegibles para cobertura de salud. Pero defensores que trabajan con inmigrantes dicen que el estado enfrenta un desafío: deshacer los efectos paralizantes de las políticas de la administración Trump, que aumentaron los temores de algunos —incluso de aquellos que son elegibles— de que inscribirse para obtener seguro de salud podría poner en peligro su capacidad, o la de un miembro de su hogar, de permanecer en el país.
“Por temor a las posibles repercusiones, ya sea ahora o en futuros trámites migratorios, las personas que tal vez habían pensado en buscar beneficios de salud volvieron a vivir en las sombras”, dijo María Albañil-Rangel, gerenta de políticas y promoción de Tri-County Health Network, con sede en Telluride, Colorado, una organización sin fines de lucro que trabaja para aumentar el acceso a la atención médica. “Se perdió la confianza. Se necesita tiempo para reconstruir eso”.
KHN trabajó con Colorado News Collaborative para examinar el progreso del estado en los últimos años para abordar las desigualdades raciales y étnicas, incluyendo la salud.
El Departamento de Salud del estado estima que alrededor del 30% de los adultos hispanos no tienen cobertura de salud. Esto contrasta con el promedio estatal del 12% de adultos de Colorado que no tienen seguro. La mayoría de los hispanos de Colorado son ciudadanos o residentes legales, pero pueden enfrentar barreras para la inscripción, incluyendo el idioma y el costo.
Las personas que viven en el país sin papeles se encuentran en un aprieto particular: en la mayoría de los estados no pueden obtener beneficios públicos —a menos que terminen en la sala de emergencias con una afección potencialmente mortal— ni tampoco comprar un seguro médico en los mercados establecidos por la Ley de Cuidado de Salud a Bajo Precio (ACA).
Según KFF, aproximadamente un tercio de los residentes hispanos sin seguro menores de 65 años no son elegibles para la cobertura de ACA, Medicaid o el Programa de Seguro de Salud Infantil (CHIP) debido a su estatus migratorio.
Colorado ha tomado medidas para cambiar esto para grupos específicos de residentes indocumentados que viven en hogares de bajos ingresos.
Una ley aprobada recientemente brindará cobertura de Medicaid y CHIP a embarazadas y niños comenzando en 2025.
A partir del próximo año, una ley aprobada en 2020 utilizará fondos estatales para ayudar a algunos residentes que viven por debajo del nivel federal de pobreza ($13,590 anuales para una persona sola o $27,750 anuales para una familia de cuatro, en 2022) a comprar seguro médico en el mercado individual.
Y en 2019, Colorado se unió a una docena de estados que cubren la diálisis regular para personas que, de otra manera, tendrían que esperar hasta estar tan enfermas que deberían ir a una sala de emergencias.
“Ya no tenemos 130 pacientes que pasan por el servicio de urgencias que necesitan diálisis de emergencia”, dijo la doctora Lilia Cervantes, directora de salud para inmigrantes de la Facultad de Medicina de la Universidad de Colorado, y principal defensora de este cambio en el servicio de diálisis, que le ha ahorrado al estado alrededor de $10 millones al año, según datos del departamento de financiamiento y política de atención médica estatal.
Pero a Cervantes le gustaría ver que más personas reciban la atención que necesitan en primer lugar, para prevenir el desarrollo de una afección crónica como la enfermedad renal.
Los datos confirman que, por sí solo, expandir el grupo de personas elegibles para un seguro de salud no es suficiente para abordar las inequidades en la cobertura. A nivel nacional, después de la implementación de la Ley de Cuidado de Salud a Bajo Precio, las tasas de cobertura mejoraron en todos los grupos raciales y étnicos, pero las desigualdades persistieron.
“Los hispanos tuvieron las mayores ganancias en cobertura durante ese período, lo que ayudó a reducir un poco las disparidades, pero aún así siguieron siendo significativamente más propensos a no tener seguro en comparación con los blancos [no hispanos]”, dijo Samantha Artiga, directora del Programa de Políticas de Salud y Equidad Racial para KFF. “Y luego, lo que vimos en 2017 es que las tasas de personas sin seguro comenzaron a subir de nuevo”.
Doctores, investigadores y defensores de la expansión del acceso a la salud para los inmigrantes en Colorado sospechan que el repunte estuvo relacionado con las políticas de inmigración de la administración Trump, incluyendo sus cambios en la regla de carga pública. Esta regla de larga data determina cuándo se le puede negar a alguien una tarjeta de residencia (tarjeta verde o green card) o una visa porque se considera que probablemente dependerá de los beneficios gubernamentales, o ya los está usando.
La administración Trump amplió la lista de beneficios que podrían usarse para negarle a alguien desde el estatus migratorio hasta cupones de alimentos (food stamps), Medicaid que no sea de emergencia y subsidios para la vivienda.
La investigación de Ideas42, un grupo de estudio de ciencias del comportamiento sin fines de lucro, publicada en la revista Health Affairs en 2020, encontró que el anuncio de los cambios de la administración Trump a la regla de carga pública se asoció con una disminución a nivel nacional en la inscripción a Medicaid, cerca de 260,000 niños menos, comparado con los niveles de 2017.
Colorado también vio caer las tasas de seguros entre hispanos. El Instituto de Salud de Colorado descubrió en una encuesta estatal que, aunque la tasa general de personas sin seguro del estado se había mantenido estable desde que se implementó ACA, las tasas de personas sin seguro entre los hispanos o latinos de Colorado habían aumentado, especialmente entre los niños.
El instituto estimó que aproximadamente el 3% de los hispanos o latinos de Colorado de 18 años o menos no tenían seguro en 2015, en comparación con aproximadamente el 8% en 2021. Entre el total de niños que eran elegibles pero no estaban inscritos en el seguro, aproximadamente la mitad eran hispanos a pesar de que componían alrededor de un tercio de todos los niños de Colorado, dijo Erin Miller, vicepresidenta de iniciativas de salud de Colorado Children’s Campaign.
En 2021, la administración Biden revirtió los cambios de carga pública que la administración Trump había implementado en 2019, y se espera que finalice una nueva regla de carga pública a finales de este año.
“Pero eso no cambia el hecho de que muchos inmigrantes realmente desconfían de lo que pueden compartir y con quién pueden compartirlo”, dijo Liz Tansey, gerente senior de Colorado Community Health Network.
Las encuestas realizadas en 2021 por la coalición de derechos de los inmigrantes Protecting Immigrant Families a familias inmigrantes, en su mayoría hispanas y asiático-americanas y de las Islas del Pacífico, encontraron que, a nivel nacional, el 40% no había oído hablar de la revocación. Casi la mitad de los encuestados cuyas familias necesitaron ayuda durante la pandemia dijeron que se negaron a presentar la solicitud por preocupaciones sobre inmigración.
El doctor Ricardo González-Fisher, oncólogo cirujano que trabaja con la organización de servicios sociales Servicios de la Raza, brinda asistencia para inscripción desde un centro de recursos de salud en el consulado de México en Denver. Más de la mitad de los inmigrantes que ve no tienen seguro. Contó que muchos de ellos le dicen que incluso si tienen seguro, no lo usarán por temor a atraer la atención equivocada. “Dicen: 'Todos nosotros tenemos al menos una o dos personas indocumentadas en nuestra casa y no queremos que nos vean’”, dijo González-Fisher.
Como resultado de las leyes estatales recientes, el seguro al que acceden los residentes de Colorado sin papeles no puede jugar en su contra en las determinaciones de carga pública, con una excepción importante: si los niños necesitan atención a largo plazo debido, por ejemplo, a discapacidades graves o enfermedades crónicas, explicó Rayna Hetlage , gerenta senior de políticas del Center for Health Progress, un grupo de defensa de la equidad en la salud con sede en Denver.
María Rodríguez, especialista en alcance y equidad en la atención médica de la División de Seguros de Colorado, es la persona clave del estado para hacer correr la voz sobre los nuevos subsidios para ayudar a las personas sin papeles a comprar un seguro médico. Ha organizado reuniones con entidades comunitarias para prepararse para la fecha de inscripción abierta del 1 de noviembre.
En el primer año del programa de subsidios, el estado puede inscribir hasta alrededor de 10,000 habitantes de Colorado indocumentados, lo que representa solo una parte de los hispanos sin papeles y sin seguro del estado.
Colorado todavía está detrás de Washington y California en cuanto a ofrecer cobertura de atención del cáncer, lo que podría haber ayudado al padre de Peniche Rosales. Sin seguro médico ni decenas de miles de dólares para comenzar el tratamiento, no pudo recibir atención hasta que encontró un hospital que lo cubriera con fondos de caridad.
La noche antes de que Peniche Rosales tuviera una entrevista con los Servicios de Ciudadanía e Inmigración de los Estados Unidos —una entrevista que le otorgaría la residencia legal— tuvo que llevar a su padre a la sala de emergencias nuevamente. Su papá le dijo que se fuera a casa y descansara.
“Estaba más preocupado por mi entrevista que por cualquier otra cosa”, dijo Peniche Rosales, quien recibió su tarjeta de residencia mientras su padre aún vivía. “Aunque sentía dolor, le dio mucha alegría”.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Armando Peniche Rosales has a crooked toe that for years has predicted the weather, growing sensitive when rain or cold is coming.
“It never healed right,” said Peniche Rosales, who broke the middle toe on his left foot as a high school soccer player in Denver years ago and limped home without seeing a doctor. He was living in the U.S. without authorization at the time. From age 9, when he moved to Denver, until he was in his 20s, he didn’t have health insurance.
The toe is a small reminder of the times his relatives felt they had “to choose between your health or your future” in the U.S., said Peniche Rosales, now 35. Both of his parents faced that decision. His mother chose her health, returning to Mexico to seek treatment for migraines and a thyroid condition, although it means she must spend a decade separated from her family. His father chose his future, working long weeks through symptoms that free clinics told him were hemorrhoids but were actually colon cancer.
Peniche Rosales’ father is now buried in a Denver cemetery with a view of the Rocky Mountains.
“He’s resting in his home, how he wanted to,” said Peniche Rosales. “He loved the mountains.”
Nationally and in Colorado, the share of people without health insurance has long been significantly higher among Hispanics than among non-Hispanic white, Black, or Asian residents. Immigrants lacking legal status and those who have legal residency but whose families have a mixture of immigration statuses make up a large portion of that group. Colorado recently made some of them eligible for health coverage, but advocates who work with immigrants say the state is up against a challenge: undoing the chilling effects of Trump administration policies that inflamed the fears of some, even those who are eligible, that signing up for health insurance could jeopardize their ability — or that of a member of their household — to stay in the country.
“People who had maybe thought about seeking out health benefits, because of a fear of possible repercussions, whether that be to them now or to future immigration status adjustments, they went back to living in the shadows,” said María Albañil-Rangel, policy and advocacy manager for the Telluride, Colorado-based Tri-County Health Network, a nonprofit working to increase health care access. “The trust is lost. It takes time to rebuild that.”
KHN worked with the Colorado News Collaborative to examine the state’s progress on addressing racial and ethnic inequities, including in health, in recent years.
The state health department estimates that about 30% of Hispanic adults have no health coverage. That contrasts with the state average of 12% of Colorado adults who don’t have insurance. Most Hispanic Coloradans are citizens or legal residents, but they can face barriers to enrollment, including language and cost.
People living in the U.S. without authorization are in a particular bind: They cannot get public benefits in most states — unless they land in the emergency room with a life-threatening condition — or buy health insurance on the Affordable Care Act marketplaces. According to KFF, about a third of uninsured Hispanic residents younger than 65 aren’t eligible for ACA coverage, Medicaid, or the Children’s Health Insurance Program because of their immigration status.
Colorado has made moves to change that for specific groups of unauthorized residents living in low-income households. A recently passed law will give Medicaid and CHIP coverage to pregnant people and children starting in 2025. Starting next year, a law passed in 2020 will use state funds to help some residents living below 138% of the federal poverty level buy health insurance on the individual market. And in 2019 the state joined about a dozen others that cover regular dialysis for people who would otherwise have to wait until they are so sick that they land in the emergency department.
“We don’t have 130 patients coming through the ED needing emergency dialysis anymore,” said Dr. Lilia Cervantes, director of immigrant health at the University of Colorado School of Medicine and the key advocate for the dialysis change, which has saved the state about $10 million a year, according to data from the state’s health care policy and financing department. But she’d like to see more people get the care they need to avoid developing a chronic condition like kidney disease in the first place.
Data bears out that, on its own, expanding the pool of people eligible for health insurance isn’t enough to address coverage inequities. Nationally, after the Affordable Care Act was implemented, coverage rates improved across racial and ethnic groups, but inequities persisted.
“Hispanic people had the largest gains in coverage over that period, which helped to somewhat narrow disparities, but they still remained significantly more likely to be uninsured compared to white people,” said Samantha Artiga, director of the Racial Equity and Health Policy Program for KFF. “And then what we saw in 2017 is that uninsured rates started creeping up again.”
Doctors, researchers, and advocates for expanding health access to immigrants in Colorado suspect the rebound was related to Trump administration immigration policies, including its changes to the public charge rule. The long-standing rule determines when someone can be denied a green card or a visa because they are deemed likely to depend on or are already using government benefits.
The Trump administration expanded the types of benefits that could be used to deny someone immigration status to food stamps, nonemergency Medicaid, and housing subsidies.
Research published by the nonprofit behavioral science group Ideas42 in the journal Health Affairs in 2020 found that the announcement of the Trump administration’s changes to the public charge rule was associated with a nationwide decrease in Medicaid enrollment of an estimated 260,000 children compared with 2017 levels.
Colorado also saw Hispanic insurance rates drop. The Colorado Health Institute found in a statewide survey that although the state’s overall uninsured rate had held steady since the Affordable Care Act was implemented, uninsured rates among Hispanic or Latino Coloradans had risen, notably among children. The institute estimated that about 3% of Hispanic or Latino Coloradans 18 and younger were uninsured in 2015, compared with about 8% in 2021. Among children who were eligible for but not enrolled in insurance, about half were Hispanic despite their making up about a third of all Colorado kids, said Erin Miller, vice president of health initiatives for the Colorado Children’s Campaign.
The Biden administration reversed the 2019 Trump administration public charge changes in 2021 and is expected to finalize a new public charge rule later this year.
“But that doesn’t change the fact that a lot of immigrants are really, really wary of what they can share and who they can share it with,” said Liz Tansey, a senior manager at the Colorado Community Health Network.
Polling from the immigrant rights coalition Protecting Immigrant Families in 2021 of mostly Hispanic and Asian American and Pacific Islander immigrant families found that nationally 40% had not heard about the reversal. Nearly half of respondents whose families needed help during the pandemic said they declined to apply because of immigration concerns.
Dr. Ricardo Gonzalez-Fisher, a surgical oncologist who works with the social services organization Servicios de la Raza, provides enrollment assistance from a health resource center in the Mexican consulate in Denver. More than half of the immigrants he sees are uninsured. He said many immigrants tell him that even if they have insurance, they won’t use it for fear of attracting the wrong kind of attention. “They say, 'All of us have at least one or two undocumented individuals in our home and we don’t want them to see us,’” Gonzalez-Fisher said.
The insurance that unauthorized Coloradans access as a result of the recent state laws cannot count against them in public charge determinations, with one important exception: if children need long-term care because of, for example, severe disabilities or chronic illnesses, said Rayna Hetlage, a senior policy manager for the Center for Health Progress, a Denver-based health equity advocacy group.
Maria Rodriguez, a health care equity and outreach specialist at the Colorado Division of Insurance, is the state’s point person for getting the word out about the new subsidies to help unauthorized people purchase health insurance. She has hosted meetings with community organizations to prepare for the Nov. 1 open-enrollment date.
In the first year of the subsidy program, the state can enroll up to about 10,000 unauthorized Coloradans, representing only a portion of the state’s unauthorized and uninsured Hispanics.
Colorado still lags behind Washington and California in offering cancer care coverage, which might have helped Peniche Rosales’ father. Without health insurance or tens of thousands of dollars to begin treatment, he couldn’t get care until he found a hospital that would cover it using charity funds.
The night before Peniche Rosales had an interview with U.S. Citizenship and Immigration Services — an interview that would grant him legal residency — he had to take his father to the emergency room again. His dad told him to go home and rest.
“He was more worried about my interview than anything else,” said Peniche Rosales. He received his green card while his dad was still alive. “Even though he was in pain, it brought him a lot of joy.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Bruce Drum posted: " Flyr (Oslo) has announced it will begin flying the Oslo - Hamburg route starting on August 15. The new route will be operated four days a week. In other news, the new airline flew a total of 149,100 guests travelled with Flyr in May, an " World Airline News
Flyr (Oslo) has announced it will begin flying the Oslo - Hamburg route starting on August 15.
The new route will be operated four days a week.
In other news, the new airline flew a total of 149,100 guests travelled with Flyr in May, an increase of 22% compared to April. The loyalty program Flyr + which was introduced in March is now counting 160,000 members. Sales are continuing to increase with 1.2 million tickets sold so far, and the last days have been averaging over 10,000 sold tickets per day.
The airline continued;
Production was 270.4 million ASK in the month, with on average nine aircraft in operation. Load factor was 62.1%, with Yield in the month of NOK 0.52.
Flyr had a regularity in operations during May of 99.4 % and punctuality of 89.7%.
Sale of tickets for the summer season continues to increase, and for June we expect a load factor up towards 80%. What we are most proud of and give us most motivation, is all the positive feedback we have received from all those who have chosen to fly with us so far, says Tonje Wikstrøm Frislid, CEO of Flyr.
Unit revenue (PASK) in May was NOK 0.34, while the average PASK from first flight in June 2021 was NOK 0.30.
Currently Flyr has a fleet of 10 aircraft, and 2 additional aircraft will be delivered during the summer. At the end of May, Flyr has 41 FTE's per aircraft, which is in line with the planned progression to reach the targeted cost level.
Besides domestic routes in Norway, the airline flies to popular sunny destinations in southern Europe:
Tech News Favs posted: " Today's featured fav is an article that will teach you how to add shortcuts to the Windows Desktop. If you use a specific program, folder or file, shortcuts will get you there conveniently and quicker. How to Add Shortcuts to the Windows Desktop -" Tech News Favs
Today's featured fav is an article that will teach you how to add shortcuts to the Windows Desktop. If you use a specific program, folder or file, shortcuts will get you there conveniently and quicker. How to Add Shortcuts to the Windows Desktop - If you want to create a desktop shortcut to a Microsoft […]
WTX News posted: "Nine in 10 people hit by rising living costs as fuel, food and energy prices surge The Independent says MORE than nine in 10 people have seen their living costs rise over the past month, as the price of food, fuel and energy continues to surge, pushing i" WTX News
The Independent says MORE than nine in 10 people have seen their living costs rise over the past month, as the price of food, fuel and energy continues to surge, pushing inflation to its highest level in four decades.
Cannabis News World posted: "Colorado Department of Agriculture Approves Two More Pesticides for Cannabis Cannabtimes <![CDATA[PRESS RELEASE - The list for pesticides that can be used on cannabis without being a violation of the Pesticide Applicators' Act has been updated. Ple" Cannabis News World
Colorado Department of Agriculture Approves Two More Pesticides for Cannabis Cannabtimes <![CDATA[PRESS RELEASE - The list for pesticides that can be used on cannabis without being a violation of the Pesticide Applicators' Act has been updated. Please note the following products have been added:IsaridGargoilTo view the updated list, click here for a pdf or click here for an Excel form. For questions regarding this change, contact Jolynn Morris at (303) 869-9060 or email jolynn.morris@state.co.us.The Colorado Department of Agriculture (CDA) is currently reviewing pesticide labels upon request and maintaining a list of products whose label it has reviewed that it believes could be used on marijuana without violating 35-10-117(1)(i), as long as the applicator follows the label directions.Please be sure to review the list; pesticide products may be removed from the allowed products list if the registrant has not renewed their pesticide product with the department. Use of unregistered pesticides on cannabis would be a violation of the Pesticide Applicators' Act.Stay InformedFor the latest information on CDA's Pesticides Program, visit these important webpages:Main Pesticides PagePesticide use in Marijuana Production]]>
WTX News posted: "Twitter chief to address London staff in mysterious meeting amid rumours of layoffs The Independent says TWITTER'S chief executive officer Parag Agrawal will be visiting the tech giant's employees in London next week. The executive, who took control " WTX News














































 Tourists were told to keep their distance.
Tourists were told to keep their distance. 







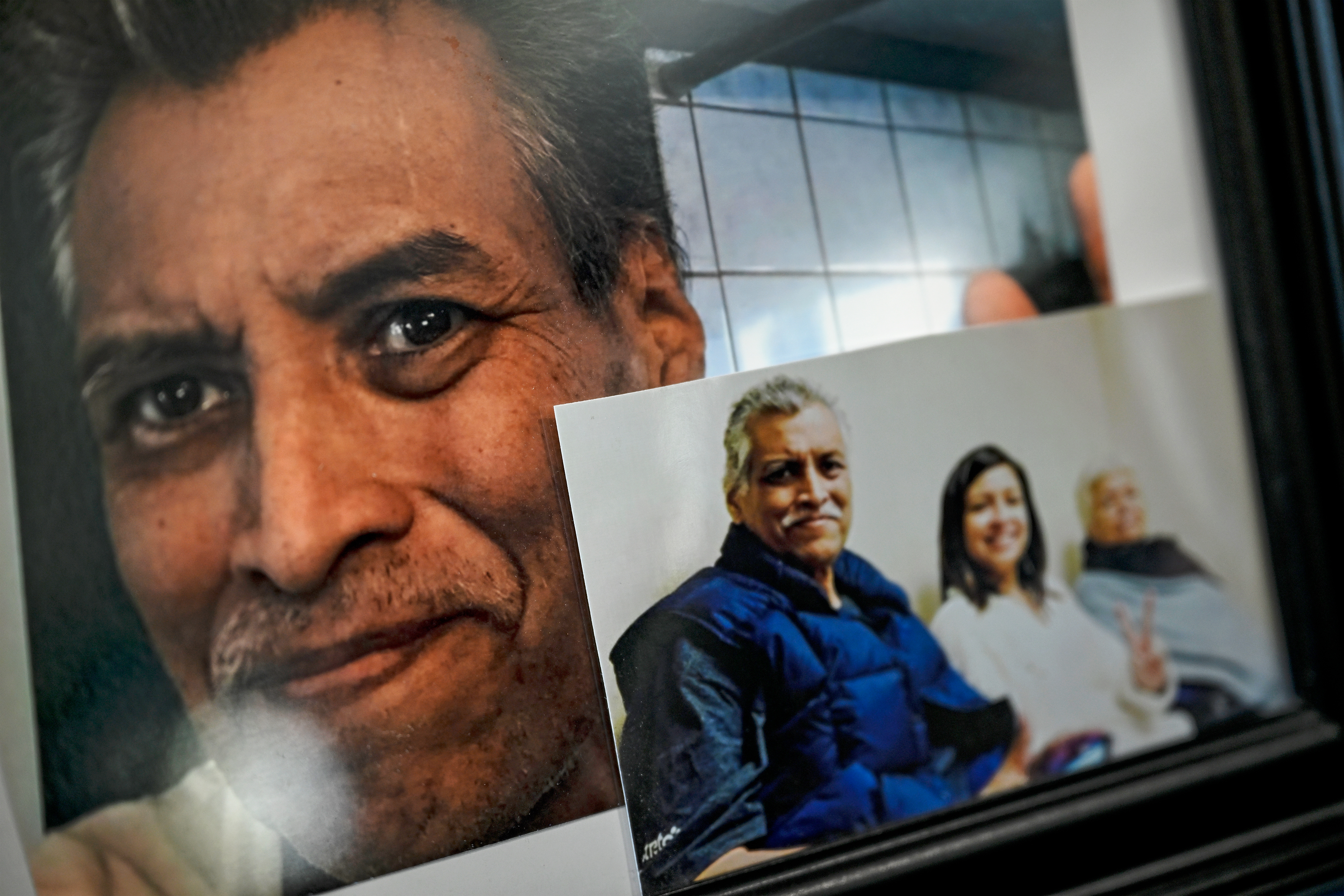












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
No comments:
Post a Comment